Research Projects
Our research focuses on disorders of the degenerative spine, with particular emphasis on lumbar and cervical spinal stenosis. Both conditions with growing societal relevance in the context of global population aging and increased functional demands up until higher ages.
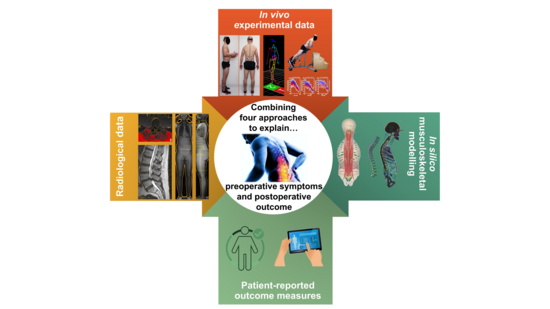
We take a translational approach that bridges basic and clinical research. At its core, our work integrates the two data sources central to clinical routine - 1. patient-reported outcomes and 2. radiological assessments (MRI, spinal alignment, disc degeneration, stenosis severity) - and expands them with objective functional and biomechanical measurements. Using 3D motion capture analysis, we characterize how spinal pathology manifests in gait, balance, postural stability, and paraspinal muscle endurance.
To gain deeper insight, we combine these methods with advanced techniques through ongoing collaborations: musculoskeletal modelling to estimate spine-internal loads and forces, and machine learning-assisted image analysis to quantify paraspinal muscle degeneration, including fatty infiltration visible on MRI.
Beyond degenerative disease, our group has dedicated expertise in spinal oncology. Prof. Netzer leads research on spinal tumors, addressing one of the most clinically complex and high-stakes areas of spine surgery.
Looking for a research project? Get in touch!
Ongoing research projects
While surgical decompression helps the majority of sLSS patients in the short term, longer-term outcomes are less predictable: symptoms recur and up to one in five patients undergoes reoperation within four years. Understanding why requires looking beyond demographics and imaging - and tracking patients well past the one-year mark.
Building on the unique dataset established in RoLSSroice I, this follow-up project extends the cohort to a 4-year postoperative follow-up and adds an age-matched asymptomatic control group for comparison. The same multimodal approach is retained - patient-reported outcomes, radiological assessment, 3D motion capture, and physical activity monitoring - now complemented by a significantly advanced modelling framework. Where RoLSSroice I used musculoskeletal modelling to estimate spinal loads, RoLSSroice II couples this with finite element modelling to capture tissue-level mechanics, including load distribution between intervertebral discs and facet joints. Patient-specific muscle geometry derived from MRI, accounting for the spatial distribution of fatty infiltration and altered muscle lines-of-action, will further improve the realism of these models.
The central aim is to develop a prediction model for mid-term surgical outcomes that integrates functional, biomechanical, and mechanistic parameters alongside conventional clinical data. To our knowledge, this represents the first multi-scale numerical modelling framework applied to lumbar spinal stenosis.
Funded by the Swiss National Science Foundation
Symptomatic lumbar spinal stenosis (sLSS) is the most common indication for spine surgery in patients over 65, yet one in four patients does not benefit meaningfully from the procedure. A key challenge is that radiological findings often fail to reflect the dynamic, activity-dependent nature of symptoms - leaving treatment decisions with limited objective guidance.
The RoLSSroice project addresses this gap through a prospective observational study following 122 patients from before surgery to one year postoperatively. Rather than relying on imaging alone, we combine patient-reported outcomes and radiological assessments with objective functional measurements: 3D motion capture analysis of gait and posture, paraspinal muscle endurance testing, surface electromyography, and wrist-worn activity monitoring. This is further complemented by musculoskeletal modelling to estimate spine-internal loads and machine learning-assisted MRI analysis to quantify paraspinal muscle degeneration.
The central goal is to identify which combination of these parameters best predicts who will benefit from surgery - and who will not. Along the way, the project is also deepening our understanding of how patients biomechanically compensate for their condition, and what role paraspinal muscle degeneration plays in this process.
Funded by the Swiss National Science Foundation
Degenerative changes at the cervical spine can lead to a narrowing of the spinal canal with consequent spinal cord compression (cervical spinal stenosis, CSS). In some cases this leads to a clinically manifested degenerative cervical myelopathy (DCM). Patients with DCM may present with different neurological signs and symptoms such as abnormal gait, balance impairments, paraesthesia, decreased fine motor skills and pain. However, the narrowing of the spinal canal does not lead to myelopathy in all patients, and less is known about the gait and balance impairments and the course of the disease of these patients.
The aims of this study are twofold. First, we aim to investigate differences in gait patterns, balance and magnetic resonance imaging (MRI) parameters of patients with CSS without signs myelopathy and patients with DCM. The presence of myelopathy has consequences on the treatment choices. Patients with DCM are typically treated surgically, while in patients with CSS without myelopathy, the first line of treatment is conservative. The second aim of this study is therefore to investigate the changes in gait patterns, balance and MRI parameters in patients treated conservatively and in patients treated surgically.
Partly supported by a grant of swissorthopaedics
Prof. Cordula Netzer's clinical and research expertise extends to spinal tumour surgery, where she is actively involved in shaping treatment standards and clinical guidelines at both national and international levels.
A central pillar of this work is her role as Steering Board Member of the AO Spine Knowledge Forum Tumor/ AOKF Tumor. This is a global clinical research group and network of leading spine surgeons advancing spine oncology care worldwide. In this capacity, she leads and supports large-scale registry-based studies, including the MTRON (Metastatic Tumor Research and Outcomes Network). This international collaboration aims to implement physician-driven landmark clinical studies, advance patient care through multicenter analysis and peer-reviewed publications, with a focus on both metastatic and the very rare primary spine tumors.
At the regional level, Prof. Netzer founded the Kompetenznetzwerk Wirbelsäulenmetastasen (Competence Network for Spinal Metastases) at University Hospital Basel, dedicated to improving multidisciplinary care for patients with spinal metastases in northwestern Switzerland.
Through this combination of international registry research and regional clinical leadership, her work bridges evidence generation and its direct translation into better outcomes for patients with spinal tumours.
Completed Projects
Low back pain is one of the most prevalent musculoskeletal disorders and a leading cause of disability worldwide. It affects up to 80% of individuals at some point in their lives. In this randomized controlled trial, we investigated whether adding an artificial intelligence (AI)-supported digital physiotherapy program to in-person physiotherapy improves the outcomes measured using questionnaires on disability, pain and quality of life in patients with nonspecific low back pain.
Study supported by Akina AG, Zurich, Switzerland
A typical symptom of symptomatic lumbar spinal stenosis (sLSS) is claudication which often leads to an early termination of walking bouts in patients. The onset of claudication differs between individuals and its causes remain unknown. Within the Walk-LSS project, we investigated whether there is an association between gait patterns (including pelvic stability), paraspinal muscle activity and the onset of symptoms that cause patients to pause during a prolonged walking test. The study included a total of 20 patients with sLSS and 20 healthy control subjects that walked for 30min (or until the symptoms caused them to stop) in a hospital hallway while lower extremity kinematics were recorded using inertial measurement units and paraspinal muscle activity was recorded using surface electromyography.
The main findings of the project were that patients walked slower than healthy controls and with altered kinematics and muscle activations. Over the duration of the walking test, muscle activation increased. However, this increase did not differ between patients and healthy controls and hence, was not specific to the onset of claudication symptoms.